Dental Implants With Gum Disease: Your 2026 Guide
- Mayde Mersal
- 2 days ago
- 7 min read


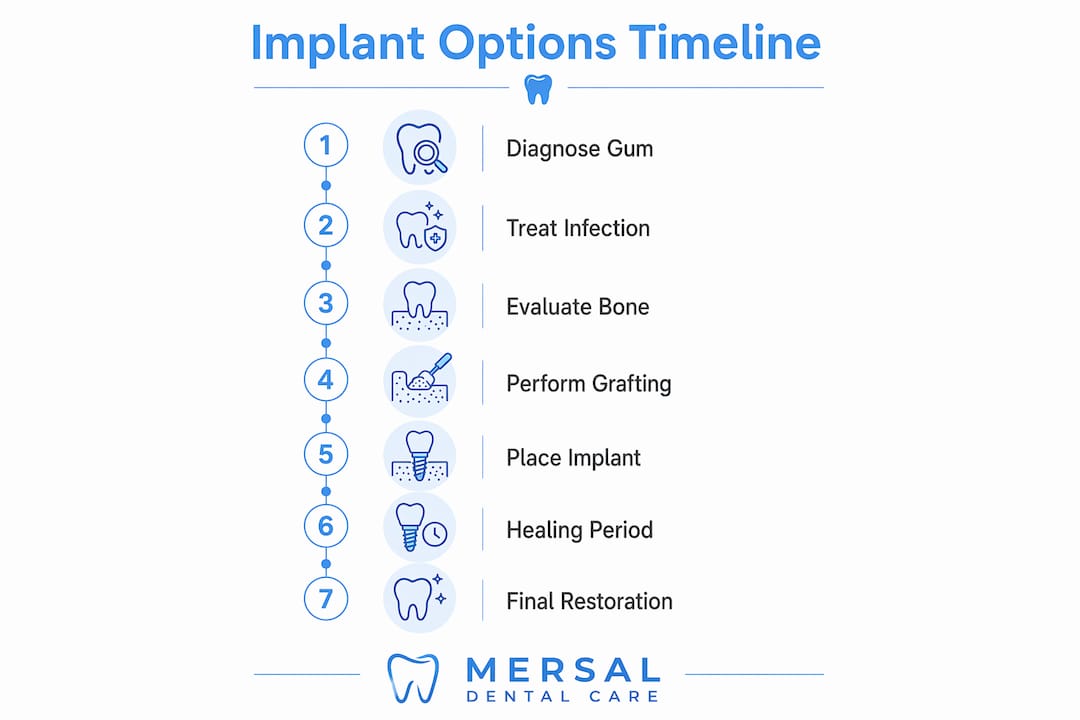
Dental implants are possible with gum disease, but only after the infection is fully treated and your gum health is stable. Active periodontal disease, the clinical term for advanced gum disease, creates a high-risk environment where implants are far more likely to fail. The bacteria driving the infection attack the same tissues that hold an implant in place. Treating the disease first is not optional. It is the single most important step between you and a successful implant.
Can you get dental implants with gum disease?
The short answer is yes, but not while the disease is active. Active untreated gum disease disqualifies you from immediate implant placement because of the high risk of peri-implantitis, an aggressive infection that destroys the bone around an implant. Your dentist or periodontist must stabilize your gum health before any implant surgery is scheduled.
Gum disease exists on a spectrum. Gingivitis is the early stage. It causes redness, swelling, and bleeding but has not yet damaged the bone. Periodontitis is the advanced stage. It destroys the bone and connective tissue that anchor your teeth. Gingivitis patients can often move toward implants relatively quickly after a professional cleaning and improved home care. Periodontitis patients require more involved treatment before they qualify.
Periodontal therapy typically includes one or more of the following:
Scaling and root planing: A deep cleaning that removes bacterial deposits from below the gumline and smooths root surfaces to prevent reattachment.
Laser gum therapy: Uses targeted energy to remove infected tissue and kill bacteria with less discomfort than traditional surgery.
Antibiotic therapy: Prescribed topically or orally to reduce bacterial load during and after mechanical treatment.
After treatment, your dental team will re-evaluate your gum health. This process takes weeks to months, depending on the severity of the disease. Only once the infection is controlled and the gums show healthy tissue response does implant planning begin.
Pro Tip: Ask your dentist for a periodontal charting report after treatment. Pocket depths of 3 mm or less signal healthy gum tissue and a green light for implant evaluation.
How does bone loss affect your implant options?
Periodontal disease does not just damage gums. It destroys the jawbone underneath. That bone is what an implant screws into. Without enough of it, a standard implant cannot be placed safely.

Standard implants require approximately 5–6 mm of bone width and 10–12 mm of bone height for secure placement. Bone loss from periodontal disease frequently leaves patients below these thresholds. The good news is that bone loss does not automatically disqualify you. Bone grafting can rebuild the site.
Bone condition | Typical next step | Healing time before implant |
Mild bone loss | Minor graft or no graft needed | 0–3 months |
Moderate bone loss | Bone graft at implant site | 3–6 months |
Severe bone loss | Larger block graft or sinus lift | 6–9 months |
Tooth still present | Socket preservation at extraction | Simultaneous healing |
Socket preservation is worth understanding. When a tooth is extracted, the surrounding bone begins to shrink almost immediately. Grafting performed at the time of extraction minimizes that shrinkage and prepares the site for a future implant without requiring a separate grafting surgery later. This approach saves time and reduces the number of procedures you need.
Several health factors influence whether grafting will succeed. Uncontrolled diabetes, smoking, and certain medications that affect bone density all reduce graft success rates. Your dental team will review your full medical history before recommending a grafting approach.
Pro Tip: If you are having a tooth extracted due to gum disease, ask about socket preservation at the same appointment. Doing both at once reduces your total recovery time significantly.
What are the implant options for severe bone loss?
When bone loss is too severe for standard implants, even after grafting, alternative techniques exist. These options are not experimental. They are well-established approaches used when conventional placement is not viable.
Zygomatic implants anchor into the cheekbone rather than the jawbone. The cheekbone is denser and largely unaffected by periodontal bone loss. This makes zygomatic implants a reliable option for patients with extreme upper jaw bone loss who would otherwise face years of grafting.
All-on-4 implant systems use four implants placed at specific angles to maximize contact with whatever bone remains. The tilted placement reaches denser bone at the back of the jaw without requiring a full graft. All-on-4 supports a full arch of teeth and is often placed the same day as extraction.
Both techniques depend on precise surgical planning. A 3D CBCT scan is the gold standard for this evaluation. It shows exact bone volume, density, and the location of critical structures like nerves and sinuses. Relying on 2D X-rays alone can lead to misjudged placement and implant failure.
The right option for you depends on:
The location and extent of bone loss
Your overall health and healing capacity
Whether you need a single tooth or full arch replacement
Your preference regarding surgery complexity and recovery time
Seeking a second opinion is always reasonable when the treatment plan is complex. Different specialists may offer different approaches, and understanding your options fully leads to better decisions. You can also review the difference between implants and bridges if you are weighing restoration alternatives.
How do you maintain implants after gum disease?
Getting an implant does not end your relationship with gum disease. Dental implants are not a cure for periodontal disease. The bacteria that caused the original infection can still attack the tissues around your implant.
The condition that results is called peri-implantitis. It behaves like gum disease but is more aggressive. Peri-implant tissue lacks the blood flow of natural tooth tissue, which means infection spreads faster and bone loss around the implant accelerates more quickly than it would around a natural tooth. Left untreated, peri-implantitis leads to implant failure.
Patients with a history of periodontal disease must follow a stricter maintenance schedule than the average implant patient. Here is what that looks like in practice:
Professional cleanings every 3–4 months. This frequency reduces bacterial buildup and catches early signs of peri-implantitis before they become serious. Standard patients typically visit every six months.
Daily interdental cleaning. Floss, interdental brushes, or a water flosser removes plaque from around the implant base where a toothbrush cannot reach.
Antibacterial mouth rinse. Chlorhexidine rinses, used as directed, reduce the bacterial load in the mouth between professional visits.
Avoiding tobacco. Smoking reduces blood flow to gum tissue and dramatically increases peri-implantitis risk. Quitting before and after implant placement improves outcomes.
Annual X-rays. Bone levels around the implant must be monitored over time to catch any early loss.
Long-term implant success depends heavily on your commitment to this maintenance routine. The implant itself does not decay. But the tissue and bone holding it in place absolutely can deteriorate without proper care. Regular dental hygiene appointments are not optional for implant patients with a periodontal history. They are what keeps the investment intact.
Pro Tip: Set a phone reminder for your 3-month cleaning appointments. Patients who treat these visits as non-negotiable have significantly better implant outcomes over the long term.
Key takeaways
Dental implants with a history of gum disease are achievable, but they require treating the disease first, rebuilding lost bone when necessary, and committing to lifelong maintenance to prevent peri-implantitis.
Point | Details |
Treat gum disease first | Active periodontal disease must be stabilized before any implant surgery is considered. |
Bone loss is manageable | Grafting and socket preservation can rebuild bone; standard implants need 5–6 mm width and 10–12 mm height. |
Alternatives exist for severe cases | Zygomatic implants and All-on-4 systems bypass the need for extensive grafting when bone loss is severe. |
3D imaging is non-negotiable | A CBCT scan provides the accurate bone assessment needed for safe implant planning. |
Maintenance is lifelong | Patients with periodontal history need professional cleanings every 3–4 months to prevent peri-implantitis. |
What I have learned treating patients with gum disease and implants
The most common misconception I see is that patients believe getting an implant solves the gum disease problem. It does not. An implant replaces a tooth. It does nothing to address the bacterial environment that destroyed the original tooth. When that misconception goes uncorrected, patients skip maintenance visits and end up losing their implant to the same disease that took their tooth.
The other challenge is treatment timelines. Patients come in hoping for a quick fix, and the honest answer is that treating gum disease, grafting bone, and placing an implant can take 12 to 18 months from start to finish in complex cases. That timeline is hard to hear. But I have seen patients go through every step and end up with implants that function beautifully a decade later. The process works when patients commit to it.
Interdisciplinary care matters here more than in almost any other area of dentistry. A periodontist, an oral surgeon, and a restorative dentist each bring something the others cannot. When those specialists communicate and coordinate, the outcomes are measurably better. If your current provider is handling everything solo without referrals, that is worth questioning.
My honest advice: do not let the timeline discourage you. Get the evaluation, understand your specific situation, and ask questions at every stage. Patients who stay engaged with their treatment plan do far better than those who hand over control and hope for the best.
— Mersal
Implant care for gum disease patients at Mersaldental
Mersaldental, located in lower town Ottawa, provides periodontal evaluation, bone grafting assessment, and implant planning for patients with a history of gum disease. We accept new patients, offer direct insurance billing, and welcome patients covered under the CDCP program. Our team coordinates every stage of care, from treating active gum disease to placing and maintaining your implant, so nothing falls through the gaps.
If you are ready to find out whether implants are right for your situation, book a consultation with our team. You can also review our full range of dental services to understand what your treatment path might look like. Same-day appointments are available for patients with urgent concerns.
FAQ
Can you get implants if you currently have gum disease?
No. Active gum disease disqualifies you from immediate implant placement because the infection dramatically increases the risk of implant failure. Treatment and stabilization must come first.
Do dental implants get infected?
Yes. Implants can develop peri-implantitis, an infection of the surrounding tissue and bone. Peri-implantitis spreads faster than natural gum disease because implant tissue has less blood flow than natural tooth tissue.
Can dental implants get cavities?
No. The implant post and crown are made from materials that do not decay. However, the gum tissue and bone around the implant can still be damaged by bacteria, which is why daily cleaning remains critical.
How long does it take to get dental implants with gum disease?
The full process typically takes 12–18 months for patients with active gum disease and bone loss. This includes periodontal treatment, bone grafting if needed, implant placement, and crown attachment.
Can you get dental implants with bone loss from periodontal disease?
Yes, in most cases. Bone grafting can restore the volume needed for standard implants, and techniques like All-on-4 or zygomatic implants are available when grafting is not sufficient.
Recommended
Comments